Neurologic symptoms in cervical spondylosis are result of a cascade of degenerative changes that most likely begin at the cervical disc
Age-related changes in chemical composition of nucleus pulposus & annulus fibrosus result in a progressive loss of their viscoelastic properties (begins from age of 21)
Disc loses height & bulges posteriorly into canal
With this loss of height, vertebral bodies drift toward one another
Posterior, there is infolding of ligamentum flavum & facet joint capsule, causing a decrease in canal & foraminal dimensions
Osteophytes form around disc margins & at uncovertebral & facet joints
Posterior protruded disc material, osteophytes, or thickened soft tissue within canal or foramen results in extrinsic pressure on nerve root or spinal cord
Mechanical distortion of nerve root may lead to motor weakness or sensory deficits
Pathogenesis of radicular pain is unclear, but is generally thought that, in addition to compression, an inflammatory response of some kind is necessary for pain to develop
Within compressed nerve root intrinsic blood vessels show increased permeability, which secondarily results in oedema of nerve root
Chronic oedema & fibrosis within nerve root can alter response threshold & increase sensitivity of nerve root to pain
Neurogenic chemical mediators of pain released from cell bodies of sensory neurons & non-neurogenic mediators released from disc tissue may play a role in initiating & perpetuating this inflammatory response
Dorsal root ganglion has been implicated in pathogenesis of radicular pain
Prolonged discharges originate from cell bodies of dorsal root ganglion as a result of brief pressure
In addition to chemicals produced by cell bodies of dorsal root ganglion, membrane surrounding dorsal root ganglion is more permeable than that around nerve root, allowing a more florid local inflammatory response
Certain arm positions may decrease stress within nerve root & relieve radicular pain
Natural History
Most patients with axial symptoms from cervical spondylosis do reasonably well:
Following 3 months of non-operative management, 70% have good to excellent relief of pain
Patients with radicular symptoms or findings have a less favourable prognosis
Disability tends to progress in patients >60 years of age
Clinical Manifestations
Symptoms are specific to a dermatomal distribution in the upper extremity, & may include sharp pain & tingling or burning sensations in involved area
There may be sensory or motor loss corresponding to the involved nerve root, & reflex activity may be diminished
Pain relief may be obtained by tilting head to the contralateral side
Shoulder abduction sign:
Relief of severe radicular pain when patient rests hand, wrist or forearm on top of head
In addition to decreasing tension within nerve root, this position may lift sensory root or dorsal root ganglion directly cephalad or lateral to source of compression, & decompression of epidural veins may contribute to pain relief
Spurling manoeuver:
Symptoms are usually aggravated by extension or lateral rotation of head to side of pain
Aggravation of symptoms by neck extension often helps to differentiate a radicular aetiology from muscular neck pain or a pathological condition of shoulder with secondary muscle pain in neck
Patients with metabolic disorders, such as diabetes, who have neuropathy may be more susceptible to radiculopathy & compressive neuropathy
Adaptations to initial radiculopathy may result in secondary pathological changes in the shoulder, carpal tunnel syndrome, or ulnar nerve irritation, which may persist long after initial radiculopathy has resolved
Neurologic deficits correspond with offending disc level in 80% of patients
Diaphragmatic involvement may result from involvement of 3rd, 4th, & 5th cervical nerve roots, manifest as paradoxical respiration
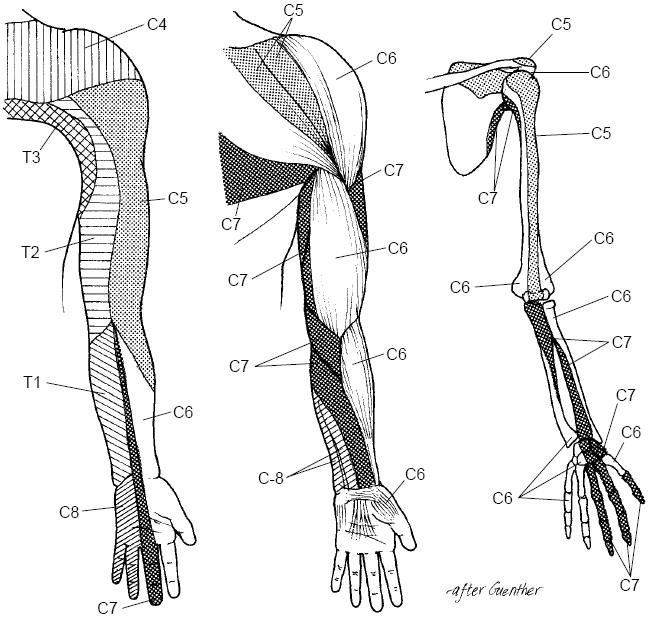
Nerve-specific radicular symptoms:
C2
Jaw pain & occipital headaches
C3
Headaches & pain along posterior aspect of neck that extends to posterior occipital region & occasionally to ear
C4
Numbness & pain at base of neck that extends to shoulder & scapular region
C5
Pain &/or numbness in an “epaulet” pattern that includes superior aspect of shoulders & lateral aspect of upper arm
Deltoid, supraspinatus, infraspinatus, elbow flexor motor function weakened
Absent biceps reflex is an inconsistent finding
C6
Pain or sensory abnormalities extending from neck to biceps region, down lateral aspect of forearm to dorsal surface of hand, between thumb & index finger, & including tips of these fingers
Sensory changes are usually restricted to below wrist
Interossei weakness
Atypical presentations:
Cervical angina
Chronic breast pain
Facial pain or paraesthesia
Dysphagia, dyspnoea, or dysphonia
Pressure on oesophagus, larynx, or trachea from marked spurring along anterior aspects of vertebral bodies as a result of proliferative degenerative changes
Wallenberg syndrome
Palsy of ipsilateral V, IX, X, & XI cranial nerves, Horner syndrome, cerebellar ataxia, & possibly death
Result of hypertrophic spurs arising from uncovertebral & facet joints occluding vertebral artery in its foramen & leading to thrombosis of vertebral artery which in turn spreads to posterior inferior cerebellar artery
Dizziness, vision blurring, tinnitus, retroocular pain, facial or jaw pain
Results from sympathetic chain involvement
Radiculopathy occasionally presents in association with myelopathy, exhibiting long tract signs
Epidural or zygapophyseal joint corticosteroid injection
Short course of cervical immobilisation in a soft collar
Prolonged immobilisation should be avoided, because cervical musculature atrophies rapidly
Duration of immobilisation should not exceed 10 days to 2 weeks & should be followed by gradual weaning
During weaning period, paraspinal muscles can be strengthened with isometric exercises
Stretching exercises can also be instituted at this time
If patient is free of pain after 6 weeks, more aggressive exercise regimens can be introduced to build up paraspinal muscles & protect neck from further attacks
Operative Management
Indications:
Persistent or recurrent radicular symptoms unresponsive to non-operative management for >6 weeks
Disabling motor weakness of <6 weeks (i.e. deltoid palsy, wrist drop)
Progressive neurologic deficit
Static neurologic deficit combined with radicular or referred pain
Instability or deformity of functional spinal unit in combination with radicular symptoms
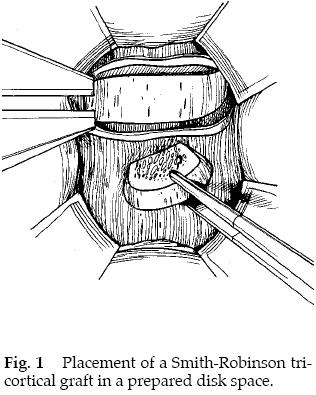
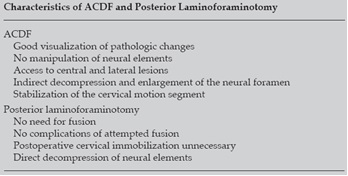
Anterior cervical discectomy & fusion:
Smith-Robinson technique
Autogenous tricortical corticocancellous horseshoe-shaped graft placed in evacuated disk space
This has now been superceded by cervical cages (titanium alloy or PEEK) which are hollowed out for the placement of autologous or synthetic bone graft, and predominantly rigidly stabilized with anterior plate fixation
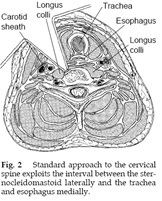
Anterolateral cervical exposure provides access from C3 to T1
Left-sided approach minimises potential risk of recurrent laryngeal palsy
A longitudinal roll is placed in interscapular area for extension
Head is positioned away from operative field, & a transverse incision is made in line with naturally occurring skin creases
A more vertical incision may be made roughly parallel to course of sternocleidomastoid if decompression of ³3 levels is anticipated
Subcutaneous tissue & platysma incised in line with skin incision
Superficial layer of deep cervical fascia is divided to expose length of sternocleidomastoid
Middle layer of deep cervical fascia is divided as carotid sheath & its contents are retracted laterally with sternocleidomastoid
Pretracheal & prevertebral layers of deep cervical fascia overlying spine are incised vertically to permit direct visualisation of vertebral body & disk spaces
Planned operative level(s) are confirmed with image intensifier (Xray)
Longus colli muscle should be elevated from cervical spine beginning at midline & proceeding bilaterally with use of a cautery for subperiosteal dissection
Longus colli should be stripped no farther laterally than point at which vertebral body curves posterior, so as to avoid injury to vertebral artery & sympathetic chain
Posterior longitudinal ligament is removed in addition to disk only if soft disk herniation posterior to it, or if ligament is part of compressive lesion, such as in ossification of posterior longitudinal ligament
Alternative to Smith-Robinson technique, for multilevel involvement, vertebrectomy & strut grafting with tricortical iliac crest or a fibular strut graft maybe undertaken
Anterior plate & screw instrumentation
Plates with screws that can be rigidly locked & that require only unicortical purchase are preferred – double screws at each level prevents potential for “windscreen wiper” effect
Decrease orthotic need, earlier functional return, & enhance fusion rate (88% for single level fusion)
Complications
Persistence of neurologic symptoms
Recurrent laryngeal nerve palsy (increased incidence with right-sided approach); manifested by hoarse voice
Thoracic duct laceration leading to chylothorax (left-sided approach)
Oesophageal laceration intra-operatively, or following hardware loosening or graft dislodgement (intravenous nutrition required until healing occurs)
Cervical sympathetic chain damage leading to Horner’s syndrome
Spinal cord penetration from over-drilling or excessive screw length
Pseudarthrosis (incidence increases with increasing number of levels attempted to fuse)
12% single level
25% multiple level
15% overall
Important to note that may not be symptomatic
Adjacent segment degeneration (<20%)
Graft donor site morbidity
Haematoma (5%)
Infection (1%)
Lateral femoral cutaneous nerve injury (10%)
Persistent iliac crest pain (15%)
Not an issue with cages
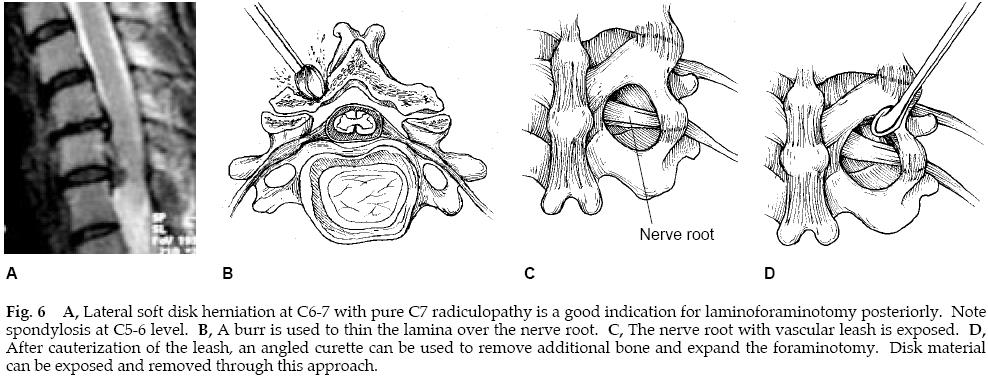
Posterior laminoforaminotomy:
Posterior approach
Prone position
Midline skin incision
Dissection to spinous processes, preserving interspinous ligament
Paraspinous muscles dissected laterally
If herniated disk material is present, nerve root is retracted superiorly to gain access to lesion
In absence of segmental kyphosis, preoperative instability, concomitant laminectomy, or excessive (>50%) facet resection, postoperative instability should not be an issue
Which surgical option?:
Factors affecting operative choice are the patient’s age, types of pathologic changes, number of motion segments involved, whether disease is unilateral or bilateral, & overall sagittal alignment
Younger patients & athletes with soft disk herniations should be considered for posterior laminoforaminotomy, as well as smokers, who are at increased risk for nonunion from ACDF
However, if radiculopathy is secondary to degenerative changes resulting in facet hypertrophy & uncovertebral-joint osteophyte formation (i.e. hard disk disease), an anterior approach may be preferable
Technical difficulties can preclude use of an anterior approach in C7-T1 disc herniations in obese or burly individuals with short necks
Patients with bilateral symptoms from a single level may be addressed with a posterior approach with bilateral keyhole laminoforaminotomy
However, bilateral foraminotomy places motion segment at increased risk for instability, & in addition, osteophyte resection is more easily & safely addressed with ACDF
Although there is some controversy, an anterior approach is preferred in cases of multilevel lateral radiculopathy
In patients without kyphosis & with less severe axial neck pain, some surgeons advocate a multiple foraminotomy because of its ease & minimal complications
However, if a laminectomy is utilised in addition to foraminotomies, development of instability & postlaminectomy kyphosis is frequent; therefore, simultaneous posterior fusion should be considered to prevent occurrence of late deformity
In general, however, cervical laminectomy is utilised only in instances of spinal cord compression in lordotic spine
There is little controversy regarding radiculopathy with midline pathologic changes, as ACDF permits surgeon to address lesions without having to manipulate spinal cord
Patients with severe axial neck pain & segmental kyphosis are optimally treated with an anterior surgical procedure