Factors implicated in development of degenerative scoliosis:
Osteoporosis
Degenerative disc disease
Osteoarthritis
Stenosis
Endochondral abnormalities
Compression fractures
Facet tropism
Lateral listhesis
Essentially 2 pathophysiologic processes result in scoliotic deformity:
Isolated degenerative arthritis of posterior facet joints to point of incompetence, when anterolisthesis develops
Asymmetric collapse of disc & asymmetric incompetence & hypertrophy of facet joints, leading to a lateral & rotational deformity; result is deformity combined with varying degrees of central lateral recess & foraminal stenosis
Natural History
Characterised by minimal structural vertebral deformities, advanced degenerative changes, & a predominance of lower lumbar curves
Distinguished from adult idiopathic scoliosis by radiographic confirmation of a straight spine during adulthood with subsequent development of a degenerative curve
Unilateral radicular symptoms much more common on side of concavity of deformity
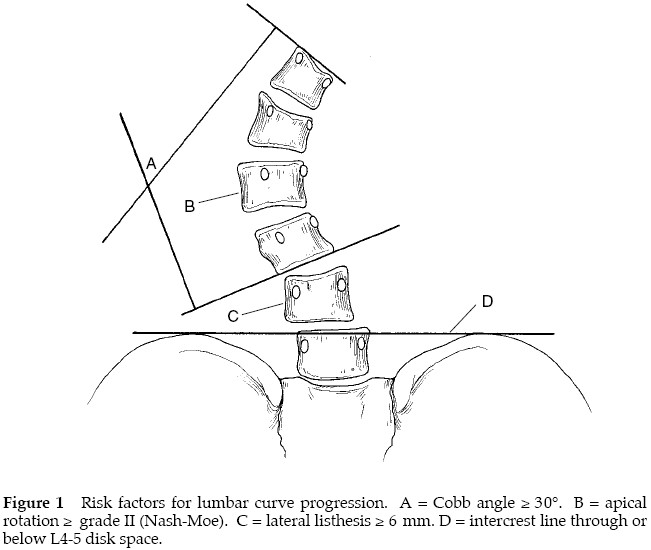
Risk factors for curve progression:
Imaging
Plain radiographs:
Patient standing without bending at knees or hips, using full-spine films to assess overall spinal balance (including EOS imaging)
Evaluated for
Curve location
Number of levels involved
Direction of curve
Magnitude of curve
Risk factors for progression
Lateral listhesis
Apical rotation
Height of residual disk spaces throughout deformity
Spondylolisthesis
Osteoporotic compression fractures
MRI:
Spinal stenosis
Management
Non-operative:
Physiotherapy
Aerobic exercise to improve cardiovascular reserve while decreasing pain & increasing function
Trunk stabilisation
NSAIDs
Paracetamol-based analgesic
Pain unit consultation
§ Tricyclic antidepressants
Night pain & can decrease neurogenic pain
§ Gabapentin/Pregabalin
May help in decreasing neurogenic pain
§ Narcotic medications
Spinal orthoses
Used primarily to control symptoms & do not stop progression of curve
Potential for pain relief must be balanced with discomfort of wearing a brace & potential for trunk muscle deconditioning
If a patient is able to function better with a brace than without, its use may be justified
Patients who use a brace should exercise regularly to avoid further deconditioning
Choice of orthosis should be based on perceived goal
Rigid lumbosacral orthosis may provide reasonable function for some patients with degenerative scoliosis
Rigid thoracolumbosacral orthosis typically would be used to help rib-to-pelvis impingement
Useful for diagnostic purposes in addition to their short-term therapeutic benefit
Operative:
Indications
Severe, refractory pain limiting ADL’s
Progressive deformity
Progressive neurologic deficits
Spinal imbalance
Decompression
Decompression & fusion
Most patients should be treated with decompression & fusion with bilateral fixation devices
Decompression alone could lead to further collapse, instability, & increased lower back & nerve pain
85% good to excellent results in terms of little to no lower extremity pain post-operatively
Surgical Recommendations
Decompression with or without fusion:
Most surgical candidates present with symptoms of neurogenic claudication, which necessitates decompression
If epidural injections provide temporary pain relief, & disc spaces through deformity are severely collapsed with no lateral listhesis or anterolisthesis, decompression alone or decompression with posterior spinal fusion without fixation devices can be considered
If more evidence of spinal instability is present, need for arthrodesis is clearer
Decompression & instrumented fusion:
In a patient with lateral listhesis >5mm, anterolisthesis, or residual disc space height with degenerative scoliosis, posterior fusion with instrumentation is reasonable
Technique also should be considered when substantial back pain accompanies neurogenic claudication
If no coronal or sagittal imbalance, fusion can be limited to levels decompressed
Fusion to sacrum is rarely indicated
If clinically significant stenosis involves L5-S1 level, a laminectomy of L5 can be done with a fusion to L5
If clinically significant spinal stenosis as well as a deformity, such as spondylolisthesis or severe foraminal stenosis at L5-S1 level, then fusion of L5 with S1 is indicated
Interbody fusion at L5-S1 level should also be considered, either through a posterior or separate anterior procedure, to structurally augment L5-S1 level & speed fusion
Deformity reconstruction:
Observation warranted with isolated or progressive deformity with minimal pain & well-maintained spinal balance
With mechanical back pain +/- neurogenic claudication, deformity is usually one of sagittal imbalance with a lumbar flat back, but it also may include elements of coronal imbalance
Decompression alone in this situation has a very high failure rate
Surgical plan should assure spinal balance &, in most cases, will require fusion to the sacrum
If deformity involves L5-S1 level, reconstruction must incorporate this level to assure spinal balance
Reconstructions often require either combined anterior & posterior approaches, multilevel posterior interbody procedures, or posterior osteotomies with fixation devices
Complications:
Occur in 20 to 40% & include
Pseudarthrosis
Wound infection
Paresthesias
Radiculopathy
CSF fistulas
Hardware failure
Compression fractures
Urinary tract infection
DVT / PE
Myocardial infarction
Adult respiratory distress syndrome
When junctional stenosis, degenerative disc disease, & progressive kyphosis proximal to fusion occur, extending proximal fusion in upper thoracic spine is justified
Fusion done 1 to 2 levels proximal to decompressed segments may ease transition to normal spine