Fit & fill of screw in isthmus of pedicle with increased screw diameter correlating favourably with pullout strength
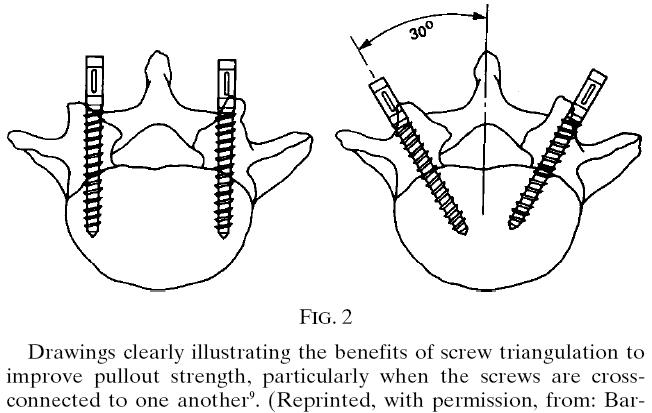
Converging screws
Patients with multiple spontaneous compression fractures are poor candidates for pedicle-screw based internal fixation because of poor bone-mineral density
Body weight is a major determinant affecting structural survival of rods used for scoliosis correction
Technique of Safe Insertion (Funnel technique)
Dorsal projection of pedicle localized
1cm-diameter section of cortical bone removed over top of pedicle with a burr or rongeur
Cancellous bone within pedicle visualized & removed with curette until pedicle cortical wall felt & visualised, followed by going deeper into pedicle toward isthmus
Kerrison rongeur used to remove cortical bone peripherally so that isthmus of pedicle can be seen
Once isthmus of the pedicle is directly palpated, a small (2mm) pedicle probe is passed through isthmus into vertebral body
Larger (5mm) probe then used to enlarge path through isthmus of pedicle
Small pins placed into probed pedicles as radiographic markers
AP & lateral images confirm pedicle path & length of screw to be used (depth of each pin measured after removal)
Threads cut into pedicle with progressively larger taps until firm cortical purchase achieved to determine screw diameter
Ball-tip probe used to feel pedicle wall viability in all directions
Screw inserted into pedicle
AP & lateral images confirm proper positioning after all of screws, rods, & connectors are inserted
Supplemental Fixation
Polymethymethacrylate may be utilised to improve fixation, esp in osteoporotic bone
Bicortical purchase routinely utilised at 1st sacral level but not at any other level
Assessment of Fusion
Radiographic demonstration of trabeculation across intertransverse (lateral) or interbody area to determine presence or absence of solid union of a spinal fusion
Union Rate
90 to 95% with pedicle-screw-based posterolateral fusion alone, without cages, using only autograft obtained from laminectomy
Complications
Nerve-root &/or cauda equina injury (5%)
Dural penetration (4%)
Deep infection (2%)
Prompt wound debridement & administration of antibiotics, with preservation of implant & subsequent delayed primary closure
Screw breakage (5%)
Screw pull-out & screw-connector disengagement
Implant-related pain
Indications
Scoliosis
Spondylolisthesis:
Vertebrectomy at 5th lumbar level with reduction of 4th lumbar onto 1st sacral vertebra with use of single-level instrumentation & fusion may be used for spondyloptosis
Spinal fracture:
1 vertebra cephalad to the damaged vertebra to 1 vertebra caudal to it
Lumbar degenerative disc disease
Spinal osteotomy
Spina bifida
Neoplasms:
Post-total vertebrectomy or radical resection
Lesions of cervical spine & cervicothoracic junction:
Traumatic & developmental lesions
Spinopelvic trauma:
Traumatic spinopelvic disruption & vertical fractures of sacrum